

As is widely known, in dental implant surgery, accurate three-dimensional positioning is essential to obtaining optimal results for a proper prosthetic rehabilitation [1]. In recent years, the combination of cone beam computed tomography (CBCT) and computer-aided design/computer-aided manufacturing (CAD/CAM) technology began to play an important role in the field of oral implantology [2]. This technology allows the production of Dent. J. 2023, 11, 123. https://doi.org/10.3390/dj11050123 https://www.mdpi.com/journal/dentistry Dent. J. 2023, 11, 123 2 of 12 different types of static surgical guides, using 3D printing technology [3,4]. As reported in a recent review, the accuracy of implant placement with computer-guided surgery has been reported in many studies (47) of traditional implantology [5]. Deviations between the virtually planned and the placed implants might represent an aggregate of errors, from imaging through data processing to guiding the placement during surgery [6,7]. However, different authors reported that digital surgical guides can improve the accuracy of implant placement [5–9].
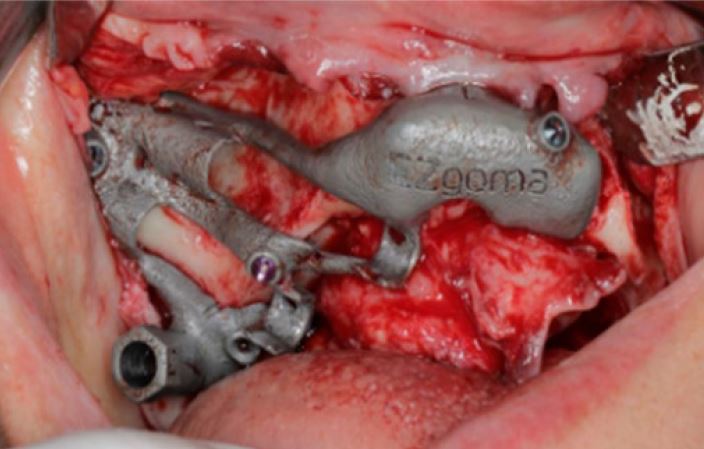
Zygomatic implant rehabilitation is an alternative treatment for patients with severe maxillary atrophy to avoid bone-lifting or grafting procedures [10]. These long implants are inserted in a region with limited space and visibility. The implant’s apex must lie completely in the zygomatic bone both to respect many anatomical limitations and to achieve the maximum bone-implant contact [11]. Hung et al. identified the posterior superior region and the central region of the zygomatic bone as suitable areas for implant tip placement [12]. In this technique, a proper position is crucial to place the ZI without functional and aesthetic complications [13]. The accuracy of the diagnostic and planning phases and the skill and experience of the operators are key factors in this surgery [14–16].
To date, guided surgery for the conventional implant is widely accepted as highprecision surgery [17–19]. For the same reason, guided surgery for the ZI based on bonesupported drill templates appears to be useful for increasing safety and accuracy [6].
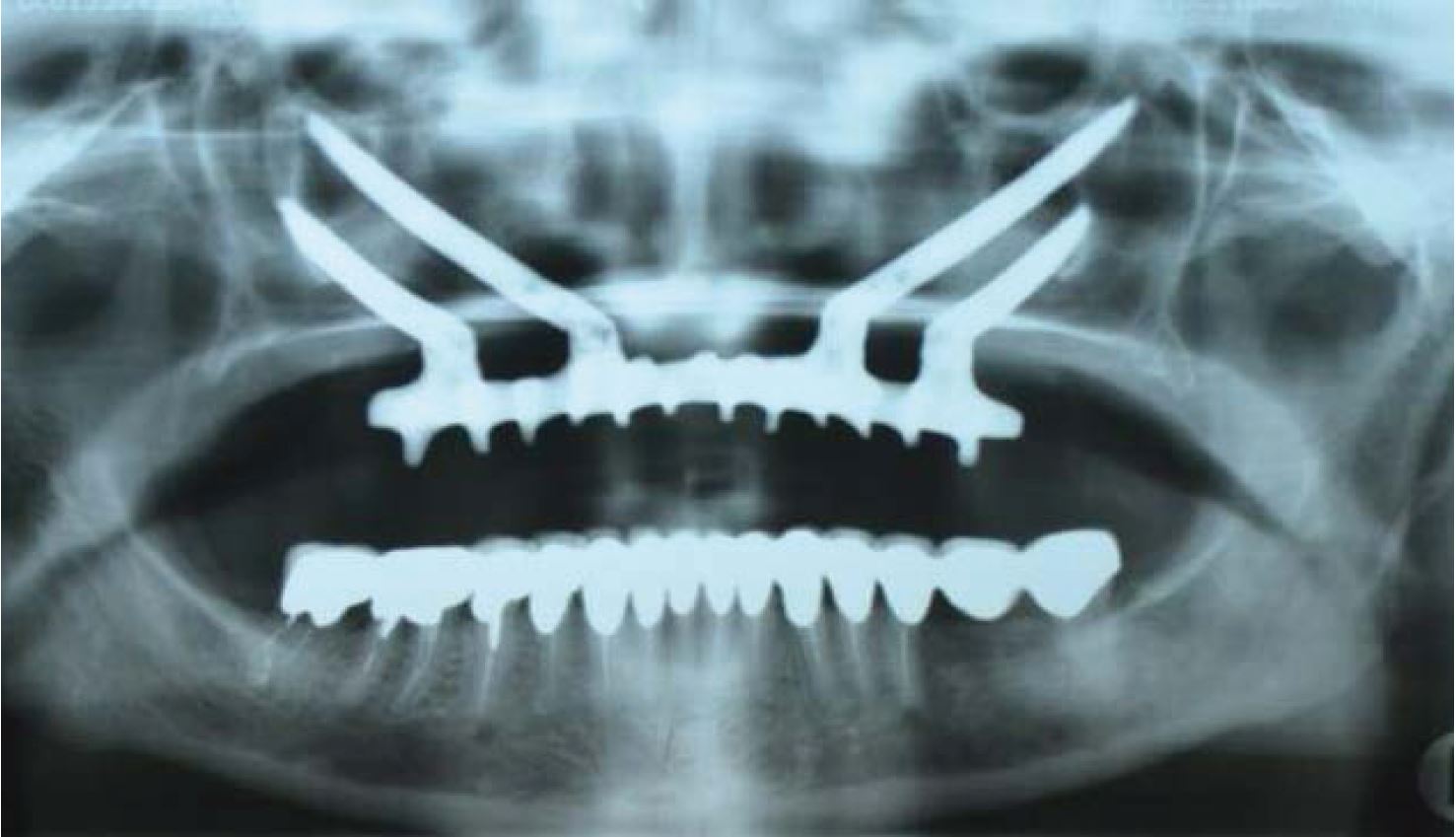
Obtaining the correct implant angulation is so crucial, especially for the multiple and contemporary ZI placements to achieve a complete restoration of the upper atrophic maxilla [20]. Discrepancies between the planned and the real implant position have become a critical point in this advanced implant surgery. Consequently, an assessment of clinical accuracy is required to determine whether guided surgery errors are clinically acceptable [21,22].
The aim of this study was to perform a three-dimensional (3D) analysis to investigate the accuracy of a novel statical surgical guide applied to zygomatic implant placement using a reliable transfer guide from a planned cooperating theatre. The primary outcome was to compare the planned and the post-operative implant positions, evaluating angular discrepancies and linear deviations in all three spatial axes. No discrepancy between the planned and placed ZIs was considered as the null hypothesis.
Zygomatic implant rehabilitation is an alternative treatment for patients with severe maxillary atrophy to avoid bone-lifting or grafting procedures [10]. These long implants are inserted in a region with limited space and visibility. The implant’s apex must lie completely in the zygomatic bone both to respect many anatomical limitations and to achieve the maximum bone-implant contact [11]. Hung et al. identified the posterior superior region and the central region of the zygomatic bone as suitable areas for implant tip placement [12]. In this technique, a proper position is crucial to place the ZI without functional and aesthetic complications [13]. The accuracy of the diagnostic and planning phases and the skill and experience of the operators are key factors in this surgery [14–16].
To date, guided surgery for the conventional implant is widely accepted as highprecision surgery [17–19]. For the same reason, guided surgery for the ZI based on bonesupported drill templates appears to be useful for increasing safety and accuracy [6].
Obtaining the correct implant angulation is so crucial, especially for the multiple and contemporary ZI placements to achieve a complete restoration of the upper atrophic maxilla [20]. Discrepancies between the planned and the real implant position have become a critical point in this advanced implant surgery. Consequently, an assessment of clinical accuracy is required to determine whether guided surgery errors are clinically acceptable [21,22].
The aim of this study was to perform a three-dimensional (3D) analysis to investigate the accuracy of a novel statical surgical guide applied to zygomatic implant placement using a reliable transfer guide from a planned cooperating theatre. The primary outcome was to compare the planned and the post-operative implant positions, evaluating angular discrepancies and linear deviations in all three spatial axes. No discrepancy between the planned and placed ZIs was considered as the null hypothesis.